Introduction
Mature cystic teratomas (MCT), also referred to as ovarian dermoid cysts, rank among the most common types of benign ovarian tumors.1 These cysts arise due to the entrapment of ectodermal components during the developmental closure of certain tissues.1 MCT’s are made up of tissues from the ectoderm, mesoderm and endoderm layers, which can include elements such as hair, skin, fat, muscle, teeth, brain tissue and even thyroid tissue.2 Dermoid cysts constitute 10–20% of all ovarian tumors and are most frequently observed in younger women, particularly around the age of 30.3
Ovarian torsion occurs when the ovary twists partially or fully around its supporting ligaments, disrupting its blood supply.4 In cases involving dermoid cysts, the likelihood of torsion is around 15%, making this a notable complication.4 As the fifth most common gynecological emergency, ovarian torsion often faces delayed diagnosis, which can lead to severe outcomes like ovarian tissue death due to infarction or necrosis.5, 6
Hemorrhagic ovarian cysts (HOCs) form when a follicular or corpus luteum cyst bleeds internally, resulting in the formation of an adnexal mass.7
Additionally, some institutions have incorporated CA 19–9 as a tumor marker for the prediction of adnexal malignancy.8
In this study a rare case of a young 22-year-old patient with the rare combination of ovarian torsion, a dermoid cyst and a hemorrhagic ovarian cyst along with elevated CA 19.9 were presented.
Case Report
A 22-year-old unmarried female presented with a 1-day history of sudden onset abdominal pain, accompanied by vomiting. The pain was severe, progressively worsening and was not alleviated by rest or medication. It was accompanied by 4 episodes of vomiting, containing food particles, non-projectile, non-bilious, non-blood tinged. There was no history of fever, vaginal discharge or burning micturition, though she did have a history of bronchial asthma for 10 years on medication.
On examination, her vital signs were as follows: pulse rate of 85 beats per minute, blood pressure of 126/80 mmHg, temperature of 97.8°F and respiratory rate of 18 breaths per minute. Abdominal examination revealed soft, tenderness and a palpable mass in the right lower quadrant. There was no guarding. Vaginal examination was normal, with no abnormal discharge or cervical motion tenderness.
Investigations
Ultrasound (USG) Abdomen and Pelvis: Revealed a complex right ovarian dermoid cyst measuring approximately 7.1 x 4.3cm with partial ovarian torsion and left hemorrhagic cyst measuring 3.1*2cm.
Blood Investigations: Haemoglobin (Hb) was 10.6 g/dL (slightly low), with a raised total white blood cell count of 16,100 cells/cu.mm, Neutrophils were 87%.
CA 19-9 Tumor Marker: Elevated to 62.8U/mL (normal <37U/mL), raising suspicion of a potential malignancy, or Chronic inflammation. β-HCG, CEA and CA-125 were normal.
Liver and renal function tests
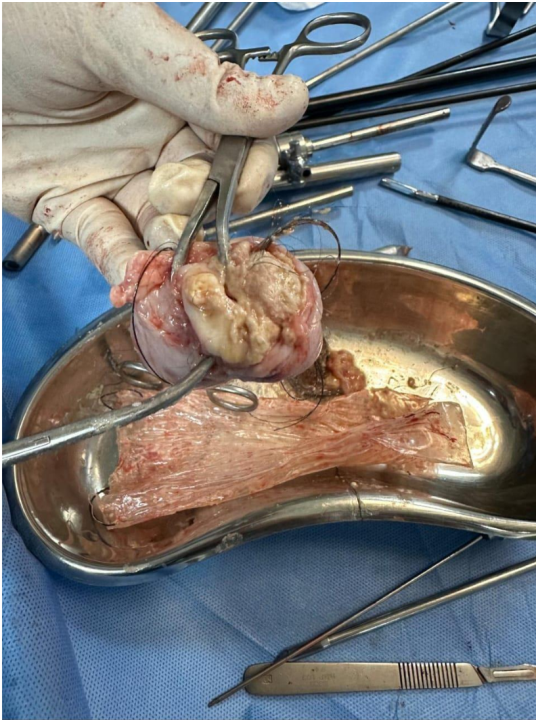
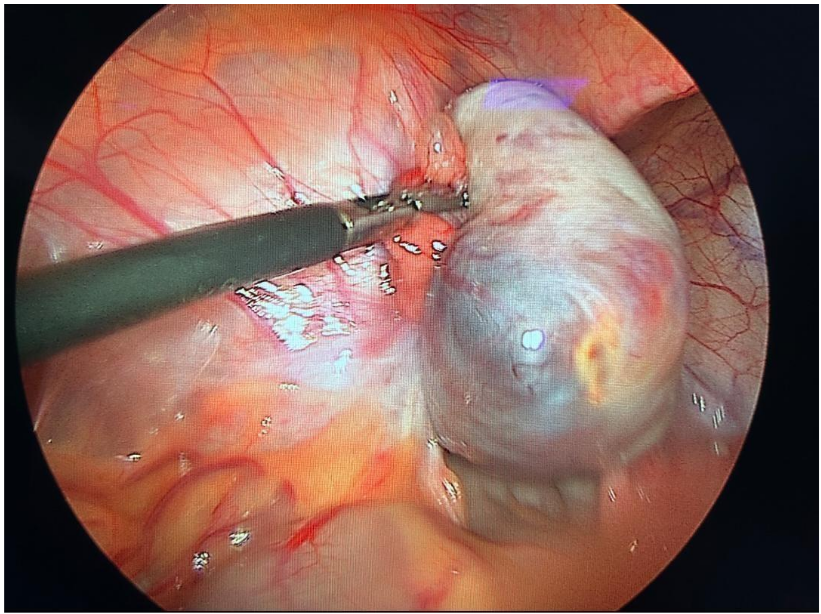
Normal, ruling out any secondary involvement Intra-operatively, Uterus was normal sized, left hemorrhagic cyst (drained 10cc of hemorrhagic fluid) and a right dermoid cyst densely adherent to the right ovary (Figure 1, Figure 2) was identified, along with torsion of the right ovary.
Based on the clinical presentation and investigation findings, the patient underwent a laparoscopic right oophorectomy (sample sent for Histopathological examination-HPE) and left cystectomy under spinal anesthesia. Peritoneal washing was performed.
Histopathological examination
Gross: Received already cut open, pale white cystic soft tissue measuring 5.9x4.5x2.9cm. External surface: Pale white, congested, smooth and glistening. Cut surface- Seen multiloculated cystic spaces filled with grey- yellow material along with hair shafts and single tooth (Rokitansky protuberance). Wall thickness ranges from 0.4 to 1.2 cm. Also seen is a cyst measuring 1.2x0.8cm. Cut surface of cyst, Clear serous fluid drained. Also noted is solid area (cartilage and bone). No residual ovarian tissue identified.
Microscopy examination
This Section studied shows ovarian tissue with multiple cysts few of which is lined by low to flattened epithelium. Also seen are cyst lined by stratified squamous epithelium with wall containing adrenal structures like sebaceous glands, eccrine ducts, apocrine glands, hair shafts. The wall also shows chronic inflammatory cell infiltrate composed of sheets of lymphocytes and plasma cells, macrophages with few hemosiderophages and multinucleated giant cells. Lumen of the cyst shows lamellated keratinous material. Also seen are cysts lined by pseudostratified ciliated columnar epithelium with foci of cartilaginous islands and bony fragments noted. No evidence of neuroepithelioma/ malignancy seen in the sections studied.
Discussion
Ovarian dermoid cysts, also known as mature cystic teratomas, are the most common form of ovarian neoplasm. These cysts develop from germ cells and can contain tissue from all three germ layers, including skin, hair, teeth and fat as well as more complex structures like bone and soft tissue.3 In our HPE, we observed the presence of hair and teeth, while microscopy revealed features such as apocrine and sebaceous glands, hair shafts, as well as deposits of bone and cartilage.
Typically, these tumors are asymptomatic and are either discovered incidentally or associated with vague symptoms.9 Malignant transformation, though rare, occurs in approximately 1–2% of cases, most often progressing to squamous cell carcinoma.9 Ovarian cystectomy is the preventive treatment in such cases.
Dermoid cysts vary in size, ranging from less than 1 centimeter to around 10 centimeters.10 In our study, the dermoid cyst measured 7 cm, placing it on the larger end of the spectrum. While it is unusual to find ovarian dermoid cysts equal to or exceeding 15 cm in diameter, especially in women of reproductive age, such cases have been reported but remain rare.11
Many women with dermoid cysts remain asymptomatic, although these cysts carry a significant risk of torsion or rupture. In rare cases, rupture can result in the release of sebaceous material into the abdominal cavity.11 In our case, we observed partial torsion of the right ovary, likely caused by the size of the cyst.
Ovarian cysts, which are fluid-filled sacs either on or within the ovary, are common, affecting roughly 20% of women during their lifetime.12 Some ovarian cysts, like hemorrhagic ovarian cysts, are particularly concerning due to the risk of rupture. When an HOC ruptures, it can lead to the release of blood and fluid into the abdomen, potentially causing severe complications such as hemoperitoneum, decreased blood flow to vital organs, or even sepsis.13 If the bleeding is extensive, emergency laparoscopic surgery may be required to control the bleeding, remove the cyst and address blood loss, which was the case for our patient.13
Predicting malignant transformation in MCTs using tumor markers has yet to be fully established.14 CA 19-9, a carbohydrate antigen commonly associated with pancreatic cancer prognosis, has been suggested as a potential marker.15 However, elevated CA 19-9 levels are not limited to malignancies. Benign conditions such as pancreatobiliary disorders, liver or lung diseases, thyroiditis, diabetes, autoimmune diseases and certain gynecological conditions like endometriosis or mucinous ovarian tumors can also cause increased CA 19-9 levels.16 In our case, the patient had a dermoid cyst. A study by Emin et al. involving 215 patients found that CA 19-9 levels were elevated in 40% of individuals with mature cystic teratomas, with average serum levels at 83.5 ± 179.2 U/mL.17
Factors such as bilaterality, cyst size the presence of fat or ectodermal elements, adhesion, rupture and necrosis from torsion have all been suggested, albeit inconsistently as possible contributors to increased CA 19-9 levels in previous studies.18 A recent study by Kyung et al. proposed that elevated CA 19-9 levels could be an indicator of ovarian torsion.19 Additionally, some researchers have hypothesized that elevated CA 19-9 levels could result from a dermoid cyst rupture, allowing the cyst’s contents to enter the bloodstream.20 A weakened cyst wall, possibly due to the large size of the cyst, may also play a role in this elevation.20
In our case, the rise in CA 19-9 levels could be attributed to several factors, including ovarian torsion, the presence of mucinous elements within the cyst, the weakened cyst wall, or its size. Malignancy could be ruled out due to the HPE findings along with the levels of tumor marker CA 19.9 returning to normal post operatively.
Conclusion
In cases of ovarian dermoid cysts in young women of reproductive age, a multidisciplinary approach is crucial for ensuring both effective treatment and fertility preservation. A team comprising gynecologists, reproductive endocrinologists, radiologists, pathologists and in some cases, oncologists can collaborate to develop a comprehensive treatment plan that considers the patient’s reproductive future, while managing the immediate risks associated with the cyst.
For fertility preservation, minimally invasive laparoscopic surgery is often favored, as it allows for the careful removal of the cyst while conserving healthy ovarian tissue. This approach is particularly important in young women, as it minimizes the risk of ovarian damage. In cases like ours, where partial ovarian torsion was caused by a large dermoid cyst, timely surgical intervention is vital to prevent ischemic damage to the ovary, which could compromise fertility. Procedures such as ovarian cystectomy focus on removing the cyst while preserving ovarian function, an important consideration for young patients.
Future studies investigating the relationship between CA 19-9 and ovarian dermoid cysts could help to better understand its diagnostic significance and improve the accuracy of pre-operative assessments, guiding clinical decision-making and potentially avoiding unnecessary concern over malignancy.
Immediate management of the cyst and longterm fertility preservation goals are addressed, providing a well-rounded care plan that balances the need for effective treatment with the patient’s reproductive aspirations.